

2025-11-05T16:27:57
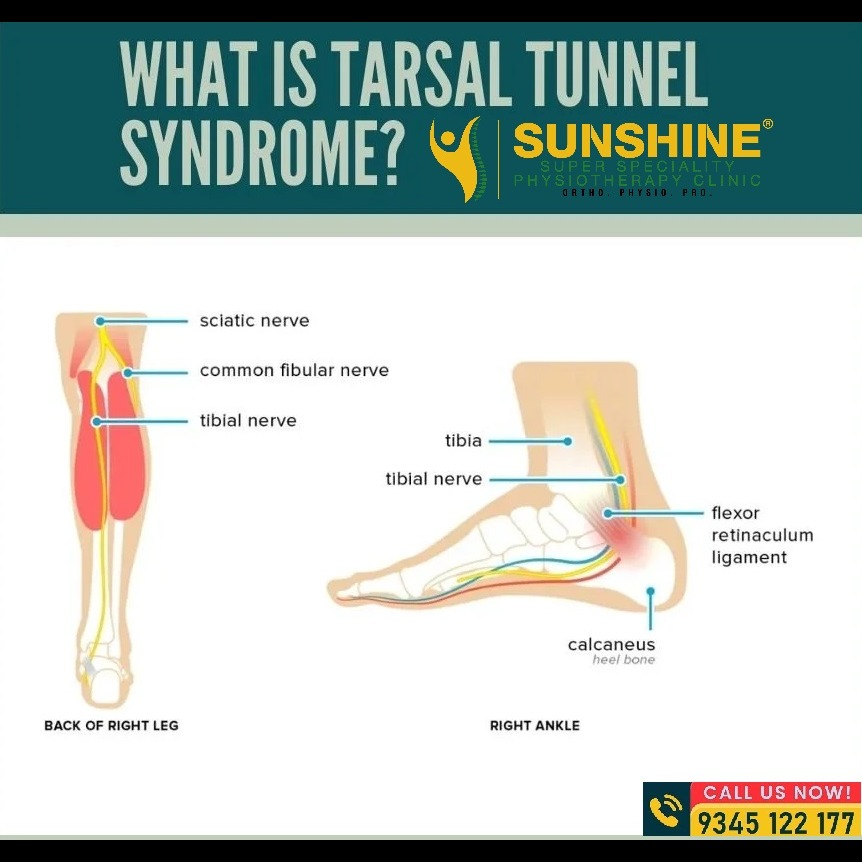
Tarsal Tunnel Syndrome (TTS): An Overview of a Complex Entrapment Neuropathy Tarsal Tunnel Syndrome (TTS), also known as 'tibial nerve dysfunction' or 'posterior tibial nerve neuralgia, ' is an entrapment neuropathy associated with the compression of structures within the tarsal tunnel at the ankle. Often compared to carpal tunnel syndrome in the wrist, TTS involves nerve compression in a confined space; however, the lower limb condition is much less common. Because TTS can mimic more frequently encountered clinical entities like plantar fasciitis and diabetic neuropathy, accurate diagnosis is crucial to prevent complications such as foot deformities and functional impairment. Anatomy and Mechanism The tarsal tunnel is a confined space supported by the surfaces of the tibia, talus, and calcaneus. It houses several essential structures: Tibialis posterior, flexor digitorum longus (FDL), and flexor hallucis longus (FHL) tendons. Posterior tibial artery and vein. Posterior tibial nerve (L4 to S3). The condition results from the compression of the posterior tibial nerve or one of its two branches—the lateral or medial plantar nerve—within the tunnel. The posterior tibial nerve typically bifurcates within the tarsal tunnel into the medial and lateral plantar nerves, though this bifurcation occurs proximal to the tunnel in about 5% of individuals. Functions of the Nerve Branches Medial plantar nerve: Provides sensory supply to the medial half of the foot and the first three foot digits. It also supplies motor innervation to the first lumbrical, abductor hallucis, flexor digitorum brevis, and flexor hallucis brevis. Lateral plantar nerve: Provides sensory innervation to the medial calcaneus and lateral heel. It also supplies motor fibers to the flexor digitorum brevis, quadratus plantae, and abductor digiti minimi. Etiology and Risk Factors TTS causes are classified as either intrinsic or extrinsic, and an impingement mechanism can be identified in approximately 80% of cases. Idiopathic TTS is rare. Intrinsic Causes Abnormalities of the tarsal tunnel structures, including: Space-occupying lesions such as varicose veins, ganglion cysts, lipomas, and neoplasms. Tendinopathy or tenosynovitis. Osteophytes, perineural fibrosis, or hypertrophic retinaculum. Extrinsic and Systemic Risk Factors Up to 43% of patients have a history of trauma, including events like ankle sprains. Abnormal biomechanics (such as excessive pronation or supination) can contribute to disease progression. Systemic diseases that pose risk factors include diabetes mellitus, hypothyroidism, gout, mucopolysaccharidosis, and hyperlipidemia. Arterial insufficiency can also lead to nerve ischemia. Epidemiology and Presentation The incidence of TTS is currently unknown, but the condition is relatively rare and often underdiagnosed. It can affect individuals at any age, but the incidence is noted to be higher in females than in males. Clinical Symptoms The predominant patient complaint is pain directly over the tarsal tunnel that radiates to the arch and plantar foot. The pain may also radiate up to the calf or higher. Common symptoms include: Sharp, shooting foot pain. Plantar numbness. Pain radiation and paresthesias along the posterior tibial nerve distribution. A tingling or burning sensation. Symptoms typically worsen at night, with standing or walking, or after physical activity, and they generally improve with rest. Dysesthesias worsening at night may disturb sleep. In severe cases, patients may experience foot muscle weakness. Physical Examination Findings Physical examination may reveal abnormalities such as pes planus, pronated foot, or talipes equinovarus. Clinicians may also observe gait abnormalities, including excessive pronation or supination, toe eversion, or an antalgic gait. Tarsal tunnel tenderness may be elicited on deep palpation. In chronic cases, signs of nerve damage include atrophy, intrinsic foot muscle weakness, and toe contractures. Strength deficits are generally considered a late finding in TTS. Diagnosis and Evaluation TTS diagnosis is often challenging because symptoms can be vague and may localize only to the medial ankle or plantar foot surface. The diagnosis is often made clinically, as no specific test exists for detecting TTS. Key Clinical Tests Tinel Test: Repeated tapping over the tarsal tunnel. A positive result—pain or tingling in the posterior tibial distribution—is a strong sign. A positive Tinel sign preoperatively is also predictive of better surgical outcomes. Dorsiflexion-Eversion Test: Passively everting and dorsiflexing the ankle and holding the position for 10 seconds. Reproduction of symptoms due to posterior tibial nerve compression is a positive sign, reported in 82% of patients with TTS. Diagnostic Studies Imaging and neurophysiological studies help rule out other conditions or identify the treatable source of symptoms. Plain Radiography (X-rays): Identifies structural abnormalities like osteophytes, tarsal coalition, hindfoot varus/valgus, or evidence of prior trauma. Ultrasound and MRI: Ultrasound allows visualization of the posterior tibial nerve and its bifurcations. Both modalities can evaluate soft tissue abnormalities such as lipomas, ganglion cysts, varicose veins, tenosynovitis, or tendonitis. MRI is not sensitive for diagnosing TTS itself but helps exclude or include other causes. Management and Treatment Management decisions (conservative versus surgical) are guided by the disease etiology, the degree of ankle and foot function loss, and the presence of muscle atrophy. Conservative Treatment The goal of conservative management, which varies in success based on etiology, is to reduce tissue stress, inflammation, and pain. Medication: Nonopioid analgesics (acetaminophen, NSAIDs) and ice are used for inflammation and pain. Neuropathic pain medications (gabapentin, pregabalin, tricyclic antidepressants) may be prescribed, along with topical NSAIDs and lidocaine. Injections: Corticosteroid injections into the tarsal tunnel can reduce edema and assist in pain relief and diagnosis. Ganglion cysts may be aspirated under ultrasound guidance. Physical Therapy & Modalities: Physical therapy may include ultrasound, iontophoresis, phonophoresis, and electrical stimulation. Nerve mobility or gliding, calf stretching, and activity modification are also recommended. Support/Orthotics: Orthotic shoes may be used to offload the tarsal tunnel and correct biomechanical abnormalities. Footwear with appropriate arch support, night splints, walking boots, or controlled ankle movement (CAM) walkers may also be trialed. Surgical Treatment Surgery is indicated if conservative management fails or if a definitive cause of entrapment is identified. Surgical management involves flexor retinaculum resection. Patients with symptoms caused by a space-occupying lesion generally respond well to surgery. Abnormally slow nerve conduction across the posterior tibial nerve is predictive of failed conservative therapy. Patients who respond best to surgical decompression tend to have a positive Tinel sign preoperatively, an early diagnosis, a clear etiology, a short history of symptoms, and no prior ankle pathology. Surgical success rates range widely, from 44% to 96%. Prognosis and Complications The prognosis of TTS varies, but the outcome is generally favorable in patients with an identifiable etiology, particularly if diagnosed early in the disease course. Patients without an identifiable cause who do not respond to conservative therapy often respond poorly to surgical intervention. Untreated or refractory TTS can result in persistent pain, as well as neuropathies of the posterior tibial nerve and its branches, leading to muscle weakness and atrophy. Postoperative complications include infection, impaired wound healing, and scar formation. In some cases, pain and other symptoms may not adequately resolve even with surgical decompression. Collaborative Care Given that TTS is a difficult and rare diagnosis, it is best managed by an interprofessional team that may include a primary care physician, orthopedic surgeon, podiatrist, radiologist, orthopedic nurse, and physical therapist. These professionals collaborate to evaluate and manage TTS, ensuring appropriate care coordination. While no specific guidelines for prevention exist, general measures include maintaining proper foot posture and alignment, strengthening foot muscles, and avoiding ankle/foot overuse. Patients who experience concerning symptoms—such as burning, tingling, numbness, or muscle weakness—should seek immediate medical help, as early intervention can help prevent progression and improve outcomes.