
2023-08-11T15:46:05
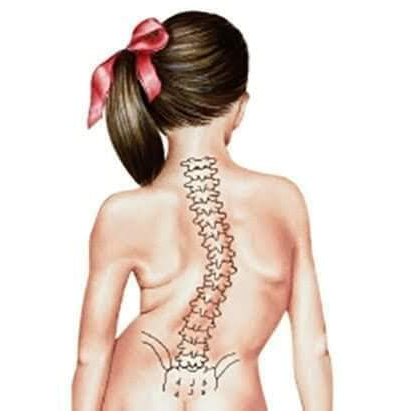
Physiotherapy clinic in Tambaram Are you Looking for Physiotherapy Treatment in Tambaram, Sunshine Super Speciality Physiotherapy Clinic, We Provide Electrotherapy, Exercise and Manual Therapy, Orthopedic, Neuro, Cardio, Pediatric, Sports and Geriatric Rehabilitation, Post Operative Physiotherapy Treatment, Fracture Rehabilitation, pain free movement. SUNSHINE ® SUPER SPECIALITY PHYSIOTHERAPY CLINIC - Scoliosis scoliosis is an abnormal lateral curvature of the spine. It is most often diagnosed in childhood or early adolescence. The spine's normal curves occur at the cervical, thoracic and lumbar regions in the so-called “sagittal” plane. These natural curves position the head over the pelvis and work as shock absorbers to distribute mechanical stress during movement. Scoliosis is often defined as spinal curvature in the “coronal” (frontal) plane. While the degree of curvature is measured on the coronal plane, scoliosis is actually a more complex, three-dimensional problem which involves the following planes: Coronal plane Sagittal plane Axial plane The coronal plane is a vertical plane from head to foot and parallel to the shoulders, dividing the body into anterior (front) and posterior (back) sections. The sagittal plane divides the body into right and left halves. The axial plane is parallel to the plane of the ground and at right angles to the coronal and sagittal planes. Scoliosis is defined by the Cobb's angle of spine curvature in the coronal plane and is often accompanied by vertebral rotation in the transverse plane and hypokyphosis in the sagittal plane. These abnormalities in the spine, costal-vertebral joints, and the rib cage produce a ‘convex’ and ‘concave’ hemithorax. The rotation component starts when the scoliosis becomes more pronounced. This is called a torsion-scoliosis, causing a gibbus. Clinically Relevant Anatomy The vertebral column normally consists of 24 separate bony vertebrae, together with 5 fused vertebrae that form the sacrum, and usually, 4 fused vertebrae that form the coccyx Spinal anatomy showing regions of the spine Regions of the spine 7 cervical vertebrae 12 thoracic vertebrae 5 lumbar vertebrae. Variations can occur such as hemi-vertebrae and fused vertebrae. When viewed from the side, the vertebral column displays five curves in the upright posture:[4] Cervical curves 2 normally occurring curves in the cervical spine: the upper cervical curve extending from the occiput to the axis, and the longer lordotic curve of the lower cervical spine extending from the axis to the second thoracic vertebrae. The upper cervical curve is convex forwards and is the reverse of the lower cervical curve. Thoracic curve Concave forwards, extending from T2 to T12. The concavity is due to the greater depth of the posterior parts of the vertebral bodies in this region. In the upper part there is often a slight lateral curve with the convexity directed to either the right or left. Lumbar curve Convex forwards and extends from L1 to the lumbosacral junction. Sacral curve Extends from the lumbosacral junction to the coccyx, anterior concavity faces downwards and forwards. Scoliosis Definition/Description Scoliosis is an abnormal lateral curvature of the spine. It is most often diagnosed in childhood or early adolescence. The spine's normal curves occur at the cervical, thoracic and lumbar regions in the so-called “sagittal” plane. These natural curves position the head over the pelvis and work as shock absorbers to distribute mechanical stress during movement. Scoliosis is often defined as spinal curvature in the “coronal” (frontal) plane. While the degree of curvature is measured on the coronal plane, scoliosis is actually a more complex, three-dimensional problem which involves the following planes: Coronal plane Sagittal plane Axial plane The coronal plane is a vertical plane from head to foot and parallel to the shoulders, dividing the body into anterior (front) and posterior (back) sections. The sagittal plane divides the body into right and left halves. The axial plane is parallel to the plane of the ground and at right angles to the coronal and sagittal planes. Scoliosis is defined by the Cobb's angle of spine curvature in the coronal plane and is often accompanied by vertebral rotation in the transverse plane and hypokyphosis in the sagittal plane. These abnormalities in the spine, costal-vertebral joints, and the rib cage produce a ‘convex’ and ‘concave’ hemithorax. The rotation component starts when the scoliosis becomes more pronounced. This is called a torsion-scoliosis, causing a gibbus. Clinically Relevant Anatomy The vertebral column normally consists of 24 separate bony vertebrae, together with 5 fused vertebrae that form the sacrum, and usually, 4 fused vertebrae that form the coccyx Spinal anatomy showing regions of the spine Regions of the spine 7 cervical vertebrae 12 thoracic vertebrae 5 lumbar vertebrae. Variations can occur such as hemi-vertebrae and fused vertebrae. When viewed from the side, the vertebral column displays five curves in the upright posture: Cervical curves 2 normally occurring curves in the cervical spine: the upper cervical curve extending from the occiput to the axis, and the longer lordotic curve of the lower cervical spine extending from the axis to the second thoracic vertebrae. The upper cervical curve is convex forwards and is the reverse of the lower cervical curve. Thoracic curve Concave forwards, extending from T2 to T12. The concavity is due to the greater depth of the posterior parts of the vertebral bodies in this region. In the upper part there is often a slight lateral curve with the convexity directed to either the right or left. Lumbar curve Convex forwards and extends from L1 to the lumbosacral junction. Sacral curve Extends from the lumbosacral junction to the coccyx, anterior concavity faces downwards and forwards. Epidemiology Scoliosis affects 2-3 percent of the population, or an estimated six to nine million people in the United States. Scoliosis can develop in infancy or early childhood. The primary age of onset for scoliosis is 10-15 years old, occurring equally among both genders. Females are eight times more likely to progress to a curve magnitude that requires treatment. Every year, scoliosis patients make more than 600, 000 visits to private physician offices, an estimated 30, 000 children are fitted with a brace and 38, 000 patients undergo spinal fusion surgery Etiology Scoliosis can be classified by etiology: idiopathic, congenital or neuromuscular. Idiopathic scoliosis The diagnosis when all other causes are excluded and comprises about 80 percent of all cases. Adult scoliosis has a prevalence of more than 8 % in adults over the age of 25 and rises up 68 % in the age of over 60 years, caused by degenerative changes in the aging spine, and a prevalence of 2, 5 % in the general population with a Cobb angle larger than 10 degrees. Adolescent idiopathic scoliosis is the most common type of scoliosis and is usually diagnosed during puberty. Classified into the following subgroups: Infantile scoliosis: Infantile scoliosis develops at the age of 0–3 years and shows a prevalence of 1 %. Juvenile scoliosis: Juvenile scoliosis develops at the age of 4–10 years, comprises 10–15 % of all idiopathic scoliosis in children, untreated curves may cause serious cardiopulmonary complications, and curves of 30 and more tend to progress, 95 % of these patients need a surgical procedure. Adolescent scoliosis: Adolescent scoliosis develops at the age of 11–18 years, accounts for approximately 90 % of cases of idiopathic scoliosis in children. Congenital scoliosis Results from embryological malformation of one or more vertebrae and may occur in any location of the spine. The vertebral abnormalities cause curvature and other deformities of the spine because one area of the spinal column lengthens at a slower rate than the rest. The geometry and location of the abnormalities determine the rate at which scoliosis progresses in magnitude as the child grows As these abnormalities are present at birth, congenital scoliosis is usually detected at a younger age than idiopathic scoliosis. Neuromuscular scoliosis Encompasses scoliosis that is secondary to neurological or muscular diseases. Includes scoliosis associated with cerebral palsy, spinal cord trauma, muscular dystrophy, spinal muscular atrophy and spina bifida. This type of scoliosis generally progresses more rapidly than idiopathic scoliosis and often requires surgical treatment. Injuries and infections to the spine can also contribute to the cause of scoliosis Characteristics/Clinical Presentation Scoliosis clinical presentation incl. x-ray Scoliosis clinical presentation incl. x-ray There are several signs that may indicate the possibility of scoliosis. Sideways curvature of the spine Sideways body posture One shoulder raised higher than the other Clothes not hanging properly Local muscular aches Local ligament pain Decreasing pulmonary function, major concern in progressive severe scoliosis. In one study, about 23 percent of patients with idiopathic scoliosis presented with back pain at the time of initial diagnosis. Ten percent of these patients were found to have an underlying associated condition such as spondylolisthesis, syringomyelia, tethered cord, herniated disc or spinal tumor. If a patient with diagnosed idiopathic scoliosis has more than mild back discomfort, a thorough evaluation for another cause of pain is advised. Due to changes in the shape and size of the thorax, idiopathic scoliosis may affect pulmonary function. Recent reports on pulmonary function testing in patients with mild to moderate idiopathic scoliosis showed diminished pulmonary function. Impairment of function was seen in more severe cases of spinal deformity, proximally-located curvature and older patients. Diagnosis Scoliosis is usually confirmed through a physical examination, an x-ray, spinal radiograph, CT scan or MRI. The curve is measured by the Cobb Method and is diagnosed in terms of severity by the number of degrees. See link .A standard exam that is sometimes used by pediatricians and in grade school screenings is called the Adam's Forward Bend Test. See link. Outcome Measures Evaluation of scoliosis treatment should include the patient’s perspective, obtained with the use of patient-reported outcome measures. SF-36 questionnaire and the EuroQol5D instrument. SRS-22 Patient Questionnaire and the quality of life profile for spinal deformities (QLPSD). The perception of the trunk deformity and body image according to the patient can be assessed by several instruments eg Walter-Reed Visual Assessment Scale (WRVAS)[8], Spinal Appearance Questionnaire (SAQ)[9], Trunk Appearance Perception Scale (TAPS)[10]. The impacts of the brace use can be measured with specific scales: Bad Sobernheim Stress Questionnaire (BSSQ) & Brace Questionnaire (BrQ). NB available instruments to evaluate the treatment for non-idiopathic scoliosis have not been sufficiently validated and analysed. Examination The aim of the functional examination is to distinguish between faulty posture and actual idiopathic scoliosis Adam Forward Bend test illustration Examination of the active movements(flexion, extension and side flexion) of the spine in the cervical, thoracic and lumbar segment. 2. The Adam forward bend test can be used to make a distinction between structural scoliosis or non-structural scoliosis of the cervical to lumbar spine. The test can be performed in the standing and sitting position. See image R .3. The Cobb angle is a standard measurement to determine and track the progression of scoliosis: see lower image R Cobb angle illustration .4. The scoliometer is an inclinometer designed to measure trunk asymmetry, or axial trunk rotation. It’s used at three areas: Upper thoracic (T3-T4) Middle thoracic (T5-T12) Thoraco-lumbar area (T12-L1 or L2-L3) If the measurement is equal to 0°, there is a symmetry at the particular level of the trunk. An asymmetry at the particular level of the trunk is found, if the scoliometer measurement is equal to any other value. 5. Pulmonary function testing is useful in the preoperative evaluation of patients. Spirometer FVC gives an assessment of lung volume FEV1 provides an assessment of flow function. Medical Management Patients with early-onset scoliosis, defined as a lateral curvature of the spine under the age of 10 years, are offered surgical treatment when the major curvature remains progressive despite conservative treatment (Cobb angle 50 degrees or more). Spinal fusion is not recommended in this age group, as it prevents spinal growth and pulmonary development. Conservative Treatment Most people with scoliosis have mild curves and probably won't need treatment with a brace or surgery. Children who have mild scoliosis may need regular checkups to see if there have been changes in the curvature of their spines as they grow. Braces Milwaukee brace When children's bones are still growing and he or she has moderate scoliosis, the doctor may recommend a brace. Wearing a brace won't cure scoliosis or reverse the curve, but it usually prevents further progression of the curve. The most common type of brace is made of plastic and is contoured to conform to the body. This brace is almost invisible under the clothes, as it fits under the arms and around the rib cage, lower back and hips. eg Milwaukee brace Most braces are worn day and night. A brace's effectiveness increases with the number of hours a day it's worn. Children who wear braces can usually participate in most activities and have few restrictions. If necessary, kids can take off the brace to participate in sports or other physical activities. Braces are discontinued after the bones stop growing. This typically occurs: About two years after girls begin to menstruate When boys need to shave daily When there are no further changes in height In general, most congenital scoliotic curves are not flexible and therefore are resistant to repair with bracing. For this reason, the use of braces mainly aims to prevent the progression of secondary curves that develop above and below the congenital curve, causing imbalance. In these cases, they may be applied until skeletal maturity. Surgical Treatment Severe scoliosis typically progresses with time A specialist may suggest scoliosis surgery to reduce the severity of the spinal curve and to prevent it from getting worse. The most common type of scoliosis surgery is spinal fusion. In spinal fusion two or more of the vertebrae are fused together, so they can't move independently. Pieces of bone or a bone-like material are placed between the vertebrae. Metal rods, hooks, screws or wires typically hold that part of the spine straight and still while the old and new bone material fuses together. If the scoliosis is progressing rapidly at a young age, surgeons can install a rod that can adjust in length as the child grows. This growing rod is attached to the top and bottom sections of the spinal curvature, and is usually lengthened every six months. Complications of spinal surgery may include bleeding, infection, pain or nerve damage. Rarely, the bone fails to heal and another surgery may be needed. Physical Therapy Management Physical therapy and bracing are used to treat milder forms of scoliosis to maintain cosmesis and avoid surgery. Scoliosis is not just a lateral curvature of the spine, it’s a three dimensional condition. To manage scoliosis work in three planes: the sagittal, frontal and transverse. Conservative therapy consists of: physical exercises bracing manipulation electrical stimulation insoles. The physical therapist has three important tasks Inform, advise and instruct. Important to do the correct exercises Inform the patient & /or parents about his/her situation. Some physical therapists recommend a brace to prevent the worsening of scoliosis. eg Milwaukee brace. Nevertheless, the evidence for bracing is controversial. There is evidence that exercises have beneficial effects on patients with idiopathic scoliosis. Physiotherapists may also address biopsychosocial factors. Adolescents who are presenting with idiopathic scoliosis and chronic low back pain symptoms may also have other factors such as insomnia, depression, anxiety and stress, and daytime sleepiness that need to be assessed and addressed as contributing factors to a chronic low back pain experience #DrParthiban #Sunshinephysioclinic.in #Physiotherapyclinicintambaram DR.M.P. PARTHIBAN.M.P.T (Ortho), Chief Orthopedic Physiotherapist, Call for Appointments: - 9345122177 East Tambaram, CHENNAI